Tonight in a nursing home in the North End neighborhood of Boston, not far from where his family owns a restaurant, there is a man with the brain of a boy. He is blind. He is 375 pounds because he doesn’t know when he is full. He can’t walk. His wheelchair is padded with a cushion from a beach chair that his mother folded in half. He has to be taken to the bathroom every thirty to sixty minutes. He can remember what his life was like before. He cries when he is asked about it.
As a boy, he and his family loved going out for breakfast and Sunday dinners. Swimming. Sports. They went to Disney World. He asks what happened to him. How long has he been here? No one tells him what happened. His mother will continue to tell him that he just arrived yesterday, that he’ll get better soon. She leaves when he goes to bed, but thinks of him in the middle of the night. When he wakes and realizes no one is there, he starts yelling loudly, like a child might, and has to be calmed. He has no short-term memory and will probably never walk again on his own. His brothers visit and take him outside.
He was twenty-five when he was incarcerated for larceny over $250 in 2005.
His name is Paul.
***
Section 30 of chapter 266 of the General Laws of the Constitution of the Commonwealth of Massachusetts states that “if the value of the property stolen exceeds two hundred and fifty dollars,” it is punishable “by imprisonment in the state prison for not more than five years, or by a fine of not more than twenty-five thousand dollars and imprisonment in jail for not more than two years.”
***
I checked in at the Middlesex Superior Court in Woburn on Tuesday, September 10. One of the court officers gave me my number, printed on a small white card, larger than the deli counter ticket but smaller than an index card. The black boldfaced number took up most of the card: 24.
After about thirty minutes, the wooden benches facing the front of the long room were lined with hundreds of legs, crossed and uncrossed, some still, others moving subtly at the ankle or forcefully at the knee. Many people drank coffee in white cups, mostly from Dunkin Donuts. Some heads bobbed, connected to iPods. Others read books. Many heads looked down at screens of varying sizes—phones, tablets, laptops. The woman beside me played Candy Crush. I read email.
The court officer joked about the Red Sox as he lowered the projection screen and left the room to start the orientation video. He told us that he knew one trial would be going to a jury immediately so he’d be back soon. Which he was, to call everyone up to and including number 76.
I followed the swarm to the courtroom on the fifth floor where the smaller group of us lined more wooden benches. It was a civil case, medical malpractice, involving a former inmate at the Billerica House of Correction. The clerk read through a list of questions. We were to raise our white card if our answer was yes and hold our cards over our heads while the officer noted the numbers for the clerk. On my left was a man who knew or was related to one of the parties or witnesses in the trial. On my right was a man I would later know as Russ.
Seven jurors had been chosen the day before. They were only looking for seven more. I raised my card three times. After most people were excused one by one, it was my turn. I made eye contact only with the judge as I explained my answers. He glanced down at my questionnaire and back at me, his hair parting to the right.
Someone in your family is or has been in law enforcement?
My uncle is a retired Watertown cop.
Do you think that would make you biased against an inmate in the Billerica House of Correction?
No.
You’ve been employed in healthcare. How?
I have worked in development for Brigham and Women’s Hospital and New England Baptist Hospital.
What’s development?
Fundraising.
Would that make you biased regarding the healthcare of an inmate?
No.
The potential length of this trial would pose a hardship?
Yes.
How?
I have two children—one is four and one is fourteen months. I only have part-time child care and I work. I am paid by the hour.
Well, it sounds like you could make it work if you need to. I’m going to empanel you for now. 
His eyes were a gentle blue, and I felt like maybe I should have tried harder to get out of it, but I couldn’t lie. I took a seat, hoping I’d be one of those randomly excused. Instead, someone else was replaced, and a few minutes later, the judge looked at us. “Ladies and gentleman,” he said, “both parties are in agreement with the jury.” I was juror number two.
We exited the courtroom through a side door and were brought to the jury deliberation room. As we rounded the conference table, a few people sat. Some had packed a snack. Some started chatting. Others read books. Some crossed their arms. I sent an email, cancelled a meeting: “The judge said this could take two weeks.”
After about twenty minutes, the court officer returned, introduced herself as Nina, and led us into the hallway to line up by number.
There are some things you can tell about a group of people in a short amount of time. From our accents, l knew all but one of us was from here. About half of us were wearing glasses. Juror number six had a wide smile whereas the man in faded jeans and work boots behind her became very serious once we were in the hall. Juror number twelve had graying hair the length of her back.
I couldn’t tell who would have answered the judge’s questions differently if they were different—if he had asked about our families, if we have sons, if we were close with our mothers, if we have anxiety, see therapists, or get migraines. He didn’t ask if we love or are related to someone who has been convicted of larceny over $250 and has been trying to get clean.
We the jury would line up in the same spots twice each day—once in the morning and once following a break—on nine of the next thirteen days. Nina led us back into the courtroom through the side door. We heard opening statements and were given instructions by the judge. We were not to discuss or research the case when court was not in session, and we were not to speak to each other about the trial. We were asked by the defense not to base our decision on sympathy.
There are other things you can learn about a group if you listen to their whispers. More than half of us were parents, more mothers than fathers. A few teachers. One electrician. One wine-seller. One was the owner of an auto body shop in the town where I grew up. One person from Everett. Framingham. Malden. Medford. Somerville. Sudbury. Westford. Some of us were from the same towns as others.
Middlesex County is the twenty-third-most-populated county in the United States, and other than eight years in Boston after college, I have been a legal resident here for all of my thirty-seven years.
***
That night, I felt anxious planning for the days ahead. Preschool drop off is at nine. Pick up is at three. Our youngest was home with me two days a week. He went to daycare three days while I worked at home a mile away. Otherwise, we’d never been apart for more than a couple of hours.
I knew everything would be fine. I wouldn’t be that far. My husband would work at home. We’d get a babysitter to help, and I would work at night. The hardest part was not knowing how many days to plan for, or which day we would potentially need to stay later to deliberate. The judge said that could be more than one day.
By the time I was on my way back to Woburn the next morning, I was excited. I realized it wasn’t a recreational venture, and I knew that the outcome was going to be sad either way, but for many reasons though none in particular, I welcomed the obligatory break from my regular work and mom-at-home routine. A leave of absence from all of the choking hazards, unrolled toilet paper, and potty talk, from all of the climbing and falling that makes my heart race through an afternoon trip to the park.
My car itself seemed to feel the pull as I accelerated onto 95. The space between my family and me grew larger, and I didn’t turn the radio down until I parked. I was a few minutes early and was going to read, but in my rearview mirror, saw my kids’ empty car seats. The weight of the silence was too heavy to sit in.
Whenever we arrived on the fifth floor, we knocked on a door to the left of the elevator, which was to the right if you took the stairs. Nina was the person to say, “All rise,” and when the court was in session, there were microphones on rather than the stenographer I’d pictured. When a sidebar was called, the lawyers chatted with the judge at his bench. The court officer turned on white noise. We spoke in whispers.
Occasionally I would look over at Dr. French, the defendant, and Mrs. Trattori, Paul’s mother. She looked like she could have been a member of my family, her olive skin and dark eyes reminding me of my sons. Dr. French, a consulting physician to a number of correctional facilities, looked over at us often. When he was not looking at us, he was looking down, using his right thumb and index finger to sort of tug at his mustache, never seeming to touch the beard. He was tall, but his posture made it seem like he wanted to appear smaller. The plaintiff’s lawyer also used his right hand to fiddle with his facial hair, but stroked the beard instead of the mustache. I wondered if there are things you can tell about men if you study the way they touch their facial hair.
***
Paul grew up in Medford. In high school, he was into boxing. He liked girls. We saw pictures of him on prom night and by the pool at his mother’s house. We saw pictures taken later, in the nursing home, in which Paul’s face is blank and his brothers are holding him up. There is a red tent around his bed. We were shown a video of a day in his life. Paul is the youngest of three: his mother’s baby.
Paul’s oldest brother testified they were a close family. Things just weren’t the same. “We can’t do the things we used to do,” he said. “It’s not easy to take him anywhere.” Their mother spends hours each day at the nursing home. She is in the photos and the video. She is happy with the care he is receiving but worried what will happen when she passes away. What if something happens to her while he is still alive?
 When he went to prison, Paul had been working at the family restaurant on and off. He had made several attempts at getting clean. While he was at the Billerica House of Correction, his brain began bleeding into itself.
When he went to prison, Paul had been working at the family restaurant on and off. He had made several attempts at getting clean. While he was at the Billerica House of Correction, his brain began bleeding into itself.
***
On Friday, September 13, I learned from the whispers around me that juror number three, who sat to my left and was about my age, had been a Marine from 1999 to 2003. He said he kicked himself for leaving, “but you know, we thought the mission was over.” Juror number one was at the finish line when the first bomb went off at the Boston Marathon. “I would have been standing right by that metal barricade you saw when they showed pictures of the suspect, but my wife wanted to get closer to the runners.”
I shook my head. “It’s all just so random.”
On my way home, I noticed that the flag at the rest stop in Lexington was at half-mast again, like it was two days earlier on 9/11. I realized that this time it was because a shooting had occurred at the Washington Naval Yard on the twelfth. Aaron Alexis had called police several weeks before because he was hearing voices. They reported this to the Navy. There were signs of a serious problem. His mother’s voice, broken, came days after the shooting. “I don’t know why he did what he did, and I’ll never be able to ask him why.”
***
I want to talk about the details of the trial now that it’s over. Things like nausea, vomiting, and mental status could be symptoms of a more serious problem. Things like vitals—blood pressure, pulse, and oxygen level—are less subjective signs. There are many kinds and causes of headache. Some headaches are symptoms of a more serious problem.
In 2005, at the Billerica House of Correction, the infirmary was located in the main building and there were modular buildings around the main building. MODS2 was the unit where inmates were housed if they were detoxing from drugs or alcohol when they entered. Within the weeks before March 14, Paul had stopped taking the Risperdal prescribed during his period of detox. His last visit with a psychiatrist was on March 11, when it was documented that Paul no longer exhibited symptoms associated with detoxification.
I learned in the research I did after the trial that, while rare, seizures are a potential side effect of Risperdal.
In 2005, at the Billerica House of Correction, it was standard practice for nurses in the infirmary to note details of visits with inmates on a green three-by-five-inch index card with lines and columns for dates and corresponding information. There was a card for each inmate and they were kept in the top drawer of a metal filing cabinet.
Exhibit one was Paul’s green card. When he went to the infirmary for the first time, as the calendar was turning from March 13 into March 14, Paul’s vitals were normal. He had taken Tylenol and Motrin in his unit. In the infirmary, he reported to Nurse Haines, the night nurse, that he felt a buzzing in his head. He had had a headache for three days. She gave him Naproxen at 1:40 a.m., and he returned to MODS2. The green card indicates that Paul was “just kidding” when he told the corrections officer that harming himself would feel better. No other symptoms were noted.
***
From the legal definition for “standard of care”:
A standard of care is a medical or psychological treatment guideline, and can be general or specific. It specifies appropriate treatment based on scientific evidence and collaboration between medical and/or psychological professionals involved in the treatment of a given condition, and applies to such things as treatment standards applied within public hospitals to ensure that all patients receive appropriate care regardless of financial means.
The medical malpractice plaintiff must establish the appropriate standard of care and demonstrate that the standard of care has been breached, with expert testimony.
***
Each expert witness is first asked to specify if and by how much they are compensated for time spent preparing for and appearing in court. In the trial of Mrs. Trattori on behalf of Paul Trattori vs. Dr. French, each side had a medical doctor, and the plaintiff had additional expert testimony. A life-care-planning consultant was paid $10,000 to gather a list of reasonable and necessary costs associated with caring for Paul for the rest of his life. A life expectancy of fifty-two took preexisting conditions into consideration.
She worked with a forensic economist, which is a position I never knew existed. A forensic economist works only in litigation. The role of this person is to use the current costs of the items associated with the life care plan to essentially place an estimated value on the rest of a patient’s life. The items listed did seem reasonable and necessary. A companion for six hours a day. A bigger wheelchair. A pillow for his wheelchair. An extra cover for the pillow, annually. Eye exams. Extra dental cleanings. Neurologist appointments. A GPS device that would tell him what intersection he is at. It all came to about eight million dollars.
***
That night at home, on the blue rocking chair in the corner of his small room, my youngest son fell asleep with his head in the crook of my left elbow, his legs across mine. I used my right hand to move his head onto my shoulder and crossed my arms under the cushion of his diaper, wriggling them closer together to feel the weight of his upper body. His thighs were chunkier now than they were when I rocked him like this for hours a day as an infant. It seemed they’d grown even pudgier in the short time we were apart.
Hearing the shift in his breathing and feeling his snores on my cheek, I carefully lowered him onto his back in the crib. As I stood, my gaze drawing a map of his body, I saw Paul’s mother folding a beach cushion in half, placing it between her son’s right hip and the metal of his wheelchair.
***
Paul returned to the infirmary for the second time at 9:50 a.m. on March 14, according to the green card. Vital signs were normal. Patient denied history of migraines. Denied symptoms such as nausea or vomiting. Denied head injury. The telephone order indicates Dr. French prescribed a higher dose of Motrin and 500 milligrams of Robaxin, a muscle relaxer. Paul returned to MODS2.
Nurse Malvo testified that she asked Paul if he hit his head or had been beaten up. He denied both. She heard a few days later from another inmate that Paul had not told her the truth. None of this is noted in the green card. She recognized her handwriting on the card, but did not write the accompanying telephone order for the prescription. The nurses worked in teams.
How a group responds to and remembers an important incident seems to tell you something about the people in that group. Over the course of the trial, none of the witnesses who worked at the Billerica House of Correction had an independent memory of Paul or of what happened to him. That is, without seeing the transcript of their deposition or the information in the exhibits, they simply did not recall Paul. They did not know how the blood began to pool in the space between his brain and his skull.
***
Since the trial has ended, I’ve been able to do some research. It seems it is common for a correctional officer to think an inmate is faking a seizure. It seems it might be common for an inmate to fake a seizure. A Google search yields articles on the subject and message boards where correctional officers share stories about their encounters with inmates. One post gives advice: “If the eyes are rolling back in the head but every once in a while they connect with you, it’s fake. If they stand up quickly when you tell them to, it’s fake.”
A sternum rub is something that can be done to check a person’s consciousness. If a person is faking a seizure, they will respond to the knuckles moving vigorously up and down the bony part of the chest. It is reported that this would be quite painful if a person is indeed conscious and responding to stimuli.
***
 Exhibit seven was the communications log kept by the correctional officers in MODS2. In 2005, their practice was to record information about incidents and inmates, in an effort to keep information flowing from one shift to the next.
Exhibit seven was the communications log kept by the correctional officers in MODS2. In 2005, their practice was to record information about incidents and inmates, in an effort to keep information flowing from one shift to the next.
During the hours contained in the days of March 11 to March 15, items about Paul were noted in the communications log that were not noted in the infirmary’s green card. Paul vomited in his cell and in the common room. He skipped chow and instead rested in his bed. He told one of the officers that he would sue him if he wasn’t taken to an outside hospital. He said that he felt like his brain was bleeding. He was not sleeping. He was complaining of a severe headache. He was being disruptive. One officer requested the inmate receive a psych visit.
Between the hours of 9:50 a.m. and 12:45 p.m. on March 14, there was a medical incident in Paul’s cell. Two correctional officers from the unit reported first, followed by two nurses from the infirmary. The first correctional officer is the one who documented the incident in the communications log. He stated the inmate was on the ground, twitching, with his eyes rolling back. When the second officer arrived, he commanded Paul to get up, saying, “I knew this was going to be you.” Paul stood up, the log states, and upon doing so, said, “Now you have to take me to the infirmary.”
Nurse McCarthy, who was Nurse Shiva’s backup, testified that when she arrived in MODS2, Paul was seated, though she was not sure if he was sitting on the floor or on the bed. He may have been seated on the footlocker, on which he said he bumped his head during the seizure.
The officer who recorded this incident noted he was “clearly faking a seizure.” Paul walked unassisted through the three traps from MODS2 to the infirmary, accompanied by Nurses Shiva and McCarthy. It was unclear how or if the pieces of information in the communications log were translated to the nurses in the infirmary or to Dr. French, the on-call physician for the approximately nine hundred inmates. No one did a sternum rub on Paul.
Faking a seizure can be a call for attention. A call for attention could be a sign of a more serious problem. Not every fake seizure is a fake.
***
In 2005, if a nurse at the Billerica House of Correction called the on-call physician, the practice would have been to report all information on the patient’s green card. If the nurse felt a patient needed to be seen by the doctor, he or she could request it. Similarly, a nurse could send a patient to the emergency room without calling the on-call physician. An inmate could put in an official request to see a doctor by filling out a sick-call form. The doctor typically visited two days each week.
The second and last time Dr. French was called about Paul’s headache was during Paul’s third trip to the infirmary at 12:45 p.m. on March 14, after the medical incident in his cell. The vital signs were normal. No other symptoms were noted. The doctor prescribed two Vicodin, the green card noted, “with question of effect.”
Nurse Malvo testified she recognized her handwriting and that “with question of effect” meant exactly that: they were unsure how the patient would respond to the medication. She didn’t recall the conversation with the doctor, didn’t know what questions he would have asked.
She didn’t remember the call on the radio that an inmate was having a seizure. She didn’t know that Paul was brought to the infirmary by Nurses Shiva and McCarthy, or that they had responded to an incident in MODS2. The first time a seizure is mentioned in the green card is many hours after Dr. French was called that last time about Paul’s headache.
***
Exhibit nine was the nurses’ communication log, similar to the correctional officers’ log. It was unclear how or if the information in this log would be translated to an on-call physician. During the time that March 14 was becoming March 15, Nurse Haines came back on duty. In the log, she noted that she received a call about Paul, being disruptive in MODS2, requesting to be transferred to the infirmary. “PLEASE NO,” she wrote. “Can Sergeant White talk to????”
She doesn’t know what she was thinking when she wrote that and she was shaky on the witness stand. Nervous. Not tearful, but emotional. Her shoulders jumped in reply to some of the questions, particularly to one of the last that the plaintiff’s lawyer asked. “You didn’t want him transferred to the infirmary, did you? You didn’t want to deal with him?”
Paul was transferred from MODS2 to the infirmary within hours of this note, at the order of a captain in the correctional unit. Nurse Haines wrote in their log, just before her shift ended at 7 a.m, that Paul was in one of the rooms, kicking the door and yelling.
The entry made in Paul’s green card at 12:30 p.m. on March 15 was in a new handwriting. Nurse Thompson had arrived earlier that morning and testified that she didn’t remember why she went to check on Paul hours later. She is the nurse who sent Paul to Saints Memorial Hospital in Lowell. His vitals were normal, but she noted his “unsteady gait and confusion.” He was transported in a cruiser instead of an ambulance. The plaintiff’s lawyer asked her if this was to get him there quicker. She said this was standard practice.
***
From the Wikipedia entry for subdural hematoma:
A subdural hematoma…also known as a subdural hemorrhage (SDH), is a type of hematoma, usually associated with traumatic brain injury. Blood gathers within the outermost meningeal layer, between the dura mater, which adheres to the skull, and the arachnoid mater, which envelops the brain. Usually resulting from tears in bridging veins which cross the subdural space, subdural hemorrhages may cause an increase in intracranial pressure (ICP), which can cause compression of and damage to delicate brain tissue. Subdural hematomas are often life-threatening when acute. Chronic subdural hematomas, however, have better prognosis if properly managed.
***
Exhibit ten was Paul’s medical record from Saints Memorial.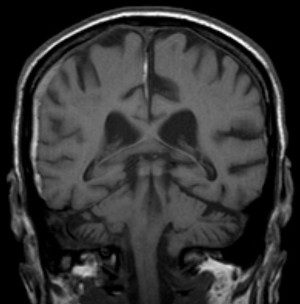
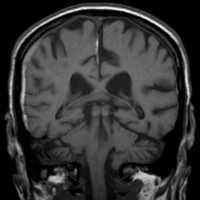
The medical expert who testified for the plaintiff explained that Paul’s blood had leaked slowly, pooling in the spaces in his skull. A CAT scan done on March 15 showed that Paul had suffered multiple strokes. The doctor testified that this was caused by a subdural hematoma, which would have likely been the result of a head trauma, which would have likely occurred five to fifteen days prior.
The only time and place that Paul reported he had hit his head on a toilet earlier in March was when he was admitted at Saints. Paul had emergency surgery to relieve the pressure, but it was too late. The expert doctor was board-certified. He used the word “blossoming” when referring to the CAT scan, explaining that once the blood had no where to go, the brain had undergone any number of strokes. The scan was one image of a flowering situation.
He testified about the various kinds of headache, the signs and symptoms that might signify something more serious. It was his opinion that Dr. French did not ask the right questions and that because the patient was male and had no history of migraines, the headache was a potential sign of something more serious. In one of his final remarks, he noted that he thought Dr. French should have called back to check on the patient. He himself would have called back to check on the patient. He didn’t know what the nurses had told Dr. French.
***
Mrs. Trattori testified. She was married in 1972 and raised her family in Medford. She used to work, but really can’t anymore. After Paul’s injury, she cared for him at home until he fell and broke his hip. Managing his care and visiting him is now her full-time job.
March 11, 2005, was the last time Mrs. Trattori spoke to the adult version of her son. We heard his pain through the recording. Paul hadn’t told the correctional officers about the headache yet. “You have to tell them,” she said.
It was at the end of her testimony that she was asked about her own health. “I have a lot of anxiety,” she said. “I get migraines myself.”
***
Each day, as I drove to the courthouse, I thought about what we might hear, which witnesses might take the stand. Sometimes it was easy to guess.
I was particularly curious to hear from the doctor. Dr. French is not board-certified, a fact to which the plaintiff’s medical expert had alluded. His lawyer asked him to explain. This was the only time the doctor showed emotion, tears forming in the corners of his eyes as he spoke slowly, shifting his focus from one member of the jury to the next. “To sit for the board exam, you need to have completed a residency,” he said. “I was accepted and started, but my mother was being treated for cancer. I didn’t have a father, and we had a two-family house. I left my residency to work in emergency rooms and clinics so I could pay the bills. I had to take care of my mother.”
He was sorry, but he did not recall Paul at all. He would remember an incident like this. He wouldn’t have prescribed Robaxin or Vicodin if he had heard of a head injury. If there were a question of a seizure, he would have advised that the patient be sent to the emergency room. If he receives two calls about a patient but not a third, he assumes the problem is resolved.
***
From an article about medical malpractice published in a medical journal:
At trial, the plaintiff’s attorney has the burden of proving every element of the case by presenting information gathered during the pretrial discovery. The attorney must convince the jury that it was more likely than not that the physician was negligent. Any assertions by the physician’s lawyer to the contrary are called defenses. Defenses serve to negate the evidence presented by the aggrieved plaintiff. The “more likely than not” standard of legal proof required in medical malpractice litigation is also called the “preponderance of evidence” standard; it is less demanding than the “beyond reasonable doubt” standard required to convict criminal defendants.
***
The trial finished on the twenty-third. It was warmer than a typical September Monday, and I figured it was my last trip up 95 to Woburn for this purpose. We were to hear closing statements, and it seemed unlikely that deliberations would go until Tuesday. I was anxious about getting back into the swing of things at home, and my nerves stepped on the gas a bit harder than usual. I arrived at the parking lot early, and instead of stealing the moments to read, I went to the jury room to chat.
Michael was a lobbyist for a teachers union. Lynn was a widow who works as a home health aid and loves seafood. Dave was the auto-body shop owner. Danielle was a real-estate agent who grew up in Sudbury but lived in Framingham. Her son was two; her daughter was six. Alexis moved from Greece when she was young. She lived in Medford and had three sons. Russ had one son in ninth grade and lived in the town where Danielle grew up. The woman who was an electrician worked for IBEW Local 103 and didn’t do side jobs: “It’s not about the money for me. I like what I do.”
Following the closing arguments, the judge explained that he chose juror number three to be our foreman because he was sure that as a high-school science teacher, John was used to keeping order. We could talk about the trial when it was over, but we weren’t to talk about the deliberations.
We’d all been curious to find out which of us would be alternates, but there were still fourteen of us. The judge did not name two of us as alternates, he said, because of his own experience serving on a lengthy jury trial only to be shunned to another room while twelve people deliberated. He keeps the jury of fourteen in each of his trials, as long as both parties’ attorneys agree it is acceptable.
***
From the same medical-journal article about medical malpractice:
Practically, “preponderance of evidence” means that an impartial jury, after hearing and considering all the information discovered by respective parties will find a greater than 50% probability that professional negligence did occur, in order to return a verdict against the physician. In this role, the jury or judge are referred to as fact-finders.
***
 Dr. French was not in the courtroom at the time of the verdict. I had seen Mrs. Trattori’s dark eyes many times over those nine days, but it was too difficult to look over as the decision was read. I didn’t know how much it would truly cost to provide a comfortable level of care for her son, and I didn’t know how her pain could be reimbursed.
Dr. French was not in the courtroom at the time of the verdict. I had seen Mrs. Trattori’s dark eyes many times over those nine days, but it was too difficult to look over as the decision was read. I didn’t know how much it would truly cost to provide a comfortable level of care for her son, and I didn’t know how her pain could be reimbursed.
We as a jury did not have to decide the value that society should place on a mother’s relationship with her son. When we answered no to the first question on the verdict form, when we decided that, given the evidence we had, Dr. French was not negligent in his care of Paul Trattori, we were instructed to skip the rest of the questions.
I cried most of the way home. Warm, sunny moments. Life one way and then another. Legs that can’t move without assistance. His mother will never know why. Did Paul get beaten up and hit his head on a toilet? What happened that he didn’t want to tell anyone? Why didn’t he fill out the form for a sick call? Why didn’t the nurses send him to an emergency room?
How is it that none of the medical staff can recall this event, at all?
***
During the trial, my fourteen-month-old started walking in earnest, finally stringing together one step and two more and then five more and so on, in the way it happens. My four-year-old is starting to sound out words. Each of these moments is stored in a treasure chest in my memory, but each milestone brings me closer to more sustained periods of time where my body is not monitoring the activities and locations of their bodies. Each moment inches forward toward less control.
How do I protect them? From all of it? I can’t vaccinate them for mental illness and addiction. I can’t know when to skip a trip to the mall or tell them they can’t go to a midnight showing of The Dark Knight. I can’t stop the space from growing.
Mrs. Trattori had a word for it: helpless.
***
I have changed the names of most of the people in this story, because we’re all innocent of something. His name is Paul. He grew up in Medford. He went to the Billerica House of Correction in 2005 after being convicted of larceny over $250.
While he was in prison, his brain bled into itself. He will live for the rest of his life in a nursing home in the North End. His mother can’t sleep, and neither can I.
***

{kind=link}
6 responses
What a terrific piece –
I recently looked up the word compassion. It means literally “to suffer with.” I am so impressed by the force of this style, by this voice which I follow now–
Beautifully written Jacqui.
Thank you! For reading and for commenting, Heather and Stephanie. Your words mean a lot. I wish I could change things for Paul, for his mother. I could not and can not but I will be thinking about them and the ways in which our system continues to fail people at the times when they need it most.
And I guess I’ll continue to fight the urge to bubble wrap my sons….thanks to The Rumpus for including my work!
This piece. Brilliant, alarming, haunting, and powerful writing. This line really hit me hard: “How do I protect them? From all of it? I can’t vaccinate them for mental illness and addiction. I can’t know when to skip a trip to the mall or tell them they can’t go to a midnight showing of The Dark Knight. I can’t stop the space from growing.” Just reading this makes it hard for me to sleep at night too. Thank you for this.
Thank you, Susie, for reading and for commenting!
Click here to subscribe today and leave your comment, or log in if you’re already a paid subscriber.